

WARNING: This story details a medical event that resulted in a patient death and may be upsetting.
It’s the sight of the blood pooling on the hospital bed, seeping through the covers, that still haunts Craig Walker.
He watched helplessly as the life drained out of his mother, her blood pressure steadily dropping, blood oozing from her body.
“I was facing the monitor. I could just see her blood pressure drop, drop, drop, drop, drop. I sort of leant on the bed and a pool of blood appeared through the sheets.”
At 11.15pm in the intensive care unit at Waikato Hospital, on a winter’s night 13 years ago, Carmen Elizabeth Walker’s heart stopped beating.
This time, the second time that day, there was no resuscitation, no frantic emergency call, no scrambling doctors and nurses, no confusion and panic.
There was only silent shock. And devastation. How did this happen?
Her husband of more than 50 years, Bob Walker, could only hold his wife’s hand and stare in disbelief as she slipped away.
On the other side of the world, Lance Walker woke to the news his beloved mum was dead. It was incomprehensible.
Rewind the clock 11 hours to 12.15pm, and Walker was being readied by ward staff for her procedure in the Harris Suite of the Radiology Department.
It was August 3, 2010. The 78-year-old Whanganui woman was undergoing an isolated limb infusion [ILI], a seemingly innocuous melanoma procedure to treat the deposits of cancer spreading up her right leg.
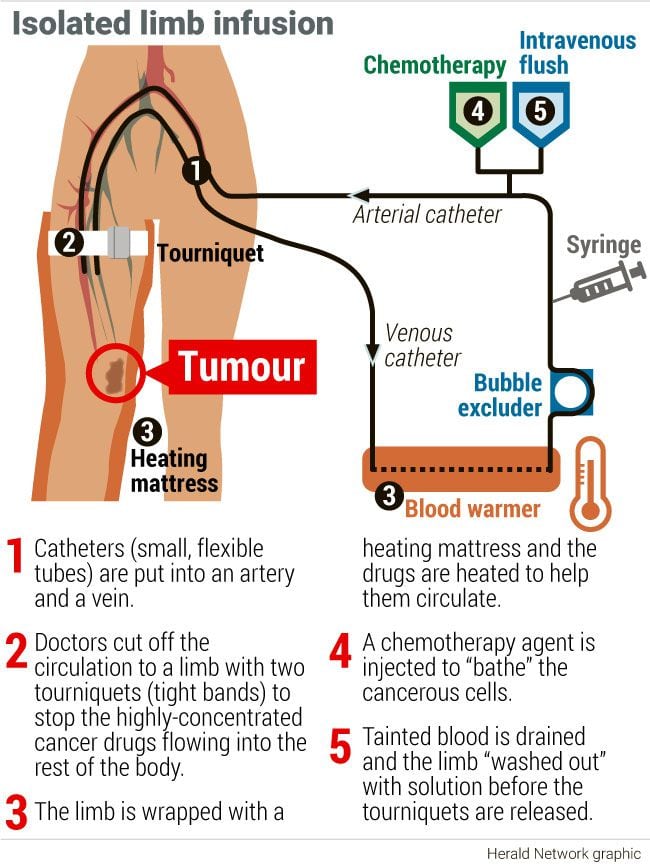
Essentially, a concentrated dose of chemotherapy is injected into the leg while it is cut off from the rest of the body’s blood circulation with a tourniquet, bathing the cancer cells, and after the drug is “washed out” the tourniquet is released.
All going well, the treatment would extend her life, and the quality of it. Walker, being an optimistic person, was confident of a good outcome.
Just as she was being wheeled from the ward, a call came through from youngest son Lance in England who wanted to wish his mother well.
“Mum was in good spirits. She said to me that she was feeling really good. She was excited and she would call me once she had finished surgery and let me know how it went.
“Not for a minute did I ever think the next call I received would be from my sister-in-law Linda, saying that something had gone wrong in surgery and Mum had died,” Lance told an inquest into Walker’s death in Hamilton last month.
“It was like a lightning bolt through the heart and I struggled to believe it as I’d only spoken to her hours before and she was so full of life. Not once did she think this would be the last hour of her life.
“Like the rest of the family, she put her trust in the surgeon and medical team as did we all.”
The procedure begins
Walker was anaesthetised at 1.15pm.
Though fit and active, she was on beta blockers for high blood pressure, had high cholesterol, heart disease, and a low haemoglobin (a protein in red blood cells that carries oxygen in the body) of 96 before the procedure indicated anaemia.
The anaesthetist in charge of her care that day, whose name is suppressed, told the inquest other than Walker requiring intermittent amounts of a type of adrenaline called metaraminol to raise her blood pressure, there were no anaesthetic concerns.
He said using such medication to maintain blood pressure was common in elderly patients with pre-existing high blood pressure.
But was this seesawing blood pressure a missed clue? An early indication of the potential for catastrophe?
/cloudfront-ap-southeast-2.images.arcpublishing.com/nzme/YFUFX32ATNFM7GJEBIP4LBMNHI.JPG) Dr Adam Greenbaum made a complaint about the care Carmen Walker received at Waikato Hospital after she died following a melanoma procedure in August 2010. Photo / Mike Scott
Dr Adam Greenbaum made a complaint about the care Carmen Walker received at Waikato Hospital after she died following a melanoma procedure in August 2010. Photo / Mike Scott
There might have been another red flag missed when radiologists struggled to insert catheters into the femoral artery of Walker’s right leg because it was so hardened by calcification.
Observing plastic surgeon Dr Adam Greenbaum, who was being primed to take over the procedure, told the inquest the chalky deposition of atherosclerosis in the walls of the artery “gave it the consistency of an incompressible clay pipe”, instead of the elastic compressibility that would allow it to be cut off by a tourniquet.
“This fatal flaw would still have been picked up if the protocol had mandated a scan after placing the catheters to check that the tourniquet worked effectively, and blood flow had been occluded,” Greenbaum told Coroner Alexander Ho.
Instead of taking the routine 30 minutes to insert the tubes needed to intravenously administer and wash out the chemo drug melphalan, it took two hours. This was “judged simply to be a technical issue”.
The surgeon, whose name is suppressed, and Greenbaum went out for coffee while the radiologists punctured Walker’s femoral artery three times with needles in search of a way in.
Retired radiologist Dr Sabaratnam Muthukumaraswamy told the inquest the needles were as wide as 3mm but he put pressure on the puncture holes to clot the blood and prevent it leaking into the thigh.
When questioned by Adam Holloway, the lawyer for the surgeon, he admitted he’d seen cases where a patient suffered a significant bleed from punctures into the femoral artery.
He also said finding a pulse in Walker’s leg, which would have indicated a leak in the tourniquet, would have been harder because of the calcification and a handheld Doppler scanner may not have worked.
When Greenbaum and the surgeon returned neither the surgeon nor the anaesthetist, who had never been involved in an ILI before, questioned why it had taken so long.
At 3.35pm, 250mg of heparin was administered to prevent blood clotting in the bypass circuit that isolated the leg from the rest of Walker’s circulation, and throughout the procedure 2500mls of fluid was infused to compensate for the temporary low blood pressure expected on release of the tourniquets.
The two stacked tourniquets were inflated and tested and the surgeon, who later admitted he was not adequately trained in ILI despite undertaking 18 of the procedures, believed they were working because he could not find a pulse in Walker’s leg.
There were also no unusual alarms in the tourniquet machine and the surgeon, who had not been in charge of an ILI for six years, did not scan for a leak.
It was then over to the perfusionist, who has name suppression and did not testify, to infuse the malphalan after which the leg was “washed out” with saline to remove the drug.
‘There’s an awful lot of blood in that bucket’
At 4.54pm the wash-out by the surgeon began.
This involved pushing a “sausage-type” exsanguinator up and down the leg until all the tainted blood and saline had been drained through the cut venous line into a purple waste bucket at the end of the bed. This was done three times.
At 5.09pm the tourniquets were deflated and Walker’s systolic blood pressure dropped from 150 millimetres of mercury to 100.
The tourniquets were temporarily reinflated, medication was administered and the systolic pressure (when the heart beats and squeezes blood into the arteries) increased to a normal 120.
On the second release, Walker remained stable and the anaesthetist injected the first dose of protamine to begin clotting the blood again.
/cloudfront-ap-southeast-2.images.arcpublishing.com/nzme/T5JDGVOWUJGDLLJ6JO75QGCIBI.JPG) Coroner Alexander Ho presided over the two-week inquest into the death of Waikato Hospital patient Carmen Walker. Photo / Mike Scott
Coroner Alexander Ho presided over the two-week inquest into the death of Waikato Hospital patient Carmen Walker. Photo / Mike Scott
Emergency anaesthetist Dr Arthur Rudman would later tell the inquest protamine was known as a “dirty drug” because it was highly anaphylactic, with one in 10 people reacting to it.
At some point, Greenbaum exclaimed, “There’s an awful lot of blood in that bucket” but said he was told by the surgeon not to worry because “a little bit of blood goes a long way”.
Greenbaum said he turned to the perfusionist and asked how he was measuring the waste fluid to know how much of it was blood and told the inquest the response was that it didn’t need to be measured because the perfusionist knew what was going in and coming out.
The perfusionist and anaesthetist both said that conversation never happened.
Within minutes Walker “collapsed”. Her blood pressure fell sharply to 50 and no amount of metaraminol, ephedrine and fluid could stabilise her.
“All I can say is there was no indication to the anaesthetic team from the surgical team, the nursing team, or the perfusionist team at this point that excessive blood had been lost,” the anaesthetist said when questioned about whether Greenbaum raised alarm at the amount of blood in the bucket.
By contrast, the surgeon said he peered in the bucket because Greenbaum had been “banging on” about the volume of blood.
Inside the bucket, a white plastic container held waste from the procedure including blood, melphalan, saline and the perfusionist’s tubing.
The surgeon thought the amount of fluid appeared normal but there was no way to measure it, short of tipping the fluid out, because he said, they had a “crap measuring system”.
The anaesthetist administered adrenaline and Walker’s blood pressure rose to 200 but moments later she “crashed” rapidly into full cardiac arrest.
Differing accounts of what happened next are complicated by the fact there are no contemporaneous notes of the 90-minute-long resuscitation - a marathon by any standards.
Greenbaum and the nurse said a crash team was called but the anaesthetist said if one was it was a mistake by the Harris Suite staff who did not understand theatre protocols.
/cloudfront-ap-southeast-2.images.arcpublishing.com/nzme/ET5T5DVH3TG2AO6ZA6CRMSLANE.jpg) Craig and his wife Linda Walker sat through sometimes gruelling details at the inquest into Carmen's death. Photo / Stuart Munro
Craig and his wife Linda Walker sat through sometimes gruelling details at the inquest into Carmen's death. Photo / Stuart Munro
The perfusionist’s evidence was that he wasn’t even in the room when Walker collapsed but Greenbaum said he and others in the crash team as well as the perfusionist, nurses and surgeon performed continuous CPR and as each peeled off for a break they wrote notes in Walker’s medical file.
He said those notes must have been removed later because they had never been seen since.
The anaesthetist denied ripping out notes and under questioning said it was not standard practice to write notes during a serious medical event unless there was a “scribe” resourced to do it.
“It would be a highly unusual and actually dangerous way of proceeding in so far as to expect the team leader ... to step away from the leadership role regularly, every time they give a drug or perform an intervention, move to the other side of a very crowded environment, write notes in the way that Dr Greenbaum has described and then return to a position of running an arrest,” he said.
“It would be a dangerous distraction from what my primary role is.”
He would rather any team working on a critically ill patient concentrate on saving the life than writing notes.
The notes could be added retrospectively, which is what he did at 8 o’clock that night.
Anaphylaxis or massive blood loss?
When Walker collapsed the anaesthetist assumed anaphylaxis or a severe adverse drug reaction to protamine was to blame.
“That’s not to say that we would not look for other causes of a cardiac arrest but that should be the first presumption on our part because if we delay that diagnosis the patient will very quickly die.”
His possible diagnoses included protamine anaphylaxis, cardio-toxicity from the melphalan, exaggerated reperfusion injury which is tissue damage caused when blood supply returns to the tissue after a lack of oxygen, hypovolaemia from excessive blood loss though he didn’t know from where, or a medical event such as a pulmonary embolism.
The protamine was halted, the anaesthetic gas withdrawn, and the advanced cardiac life support protocol initiated.
Greenbaum said the continued treatment for anaphylaxis was despite “the evidence before their eyes of many litres of blood-red fluid that had drained from Carmen’s body, to which I drew their attention”.
Rudman was called for by the anaesthetist and swiftly arrived with a transoesophageal echo machine, an ultrasound probe that showed a “very empty” left ventricle of the heart.
After that it was clear there was “no anaphylactic reaction, nor anything wrong with Carmen’s heart”, Greenbaum said.
“The problem was that her heart had nothing to pump, because all her blood had been emptied into the bucket, and so her heart was pumping against a vacuum in an empty system of arteries and veins.”
/cloudfront-ap-southeast-2.images.arcpublishing.com/nzme/GPSWLF6KEDI7RZLKOTY5KEO36E.jpg) Carmen Walker was a fit pensioner who delivered Meals on Wheels to the elderly before she was diagnosed with melanoma in her right ankle in 2009. Photo / Stuart Munro
Carmen Walker was a fit pensioner who delivered Meals on Wheels to the elderly before she was diagnosed with melanoma in her right ankle in 2009. Photo / Stuart Munro
However, the anaesthetist told the inquest while the discovery made hypovolaemia the most likely diagnosis, he considered it could be from either anaphylaxis due to fluid loss or haemorrhage.
He did not order a massive transfusion protocol, essentially an SOS to the hospital’s Blood Bank for a life-saving supply of blood products.
Greenbaum’s evidence is that the anaesthetist ordered blood, but “nowhere near enough”.
At 5.27pm, an arterial blood gas reported a haemoglobin of 65.
The anaesthetist said this low haemoglobin was consistent with Walker’s starting point of 96, the fluid he administered and the predicted loss of blood from the leg.
He and the treating team agreed anaphylaxis remained the most likely cause.
At 5.43pm, two units of red blood cells were issued.
Ten minutes later a second arterial blood gas returned a level of 28, so low a pathologist would later remark it was “incompatible with life”.
The anaesthetist immediately pivoted to blood loss as being the cause of Walker’s cardiac arrest.
“... we’ve got a haemoglobin of 28. We seem to have lost a lot of blood from somewhere. Where could that have gone because they [the surgeons] would be the only people that I imagine would recognise where that had gone...”
The surgeon looked in the bucket again and conceded maybe there was more blood after all.
Extra blood products were ordered, but by now Walker’s heart had been all but “empty” for some 40 minutes.
“Initially the blood and fluids with which Carmen’s circulation was replaced worked, but not before we replaced more than Carmen’s entire circulating blood volume,” Greenbaum said.
At 6.45pm, Walker’s jaw moved spontaneously. Was she starting to wake up?
What went wrong?
Outside the Harris Suite Bob and Craig Walker began to worry.
It was three hours since Walker’s procedure was meant to have finished and they’d had no news.
“I thought to myself ‘there’s something up here’,” Craig told NZME.
Sometime after 7pm, a nurse informed the pair they’d be taken to Walker’s room.
In the blur that followed Greenbaum and the anaesthetist appeared and informed them Walker might not survive.
“I can’t recall all the conversation. You’re just in shock. You’re basically not taking in everything they’re saying to you.”
The father and son were stunned into silence.
There had been no indication when Walker met with the surgeon weeks earlier that she could die, Bob would later tell his sons.
The surgeon disputes this and says death as a possible outcome was noted on the consent form Walker signed.
/cloudfront-ap-southeast-2.images.arcpublishing.com/nzme/IA6QKTT63JHGDBNRHUBLO7YHBM.jpg) Soulmates Bob and Carmen Walker on their wedding day. More than 50 years later Carmen would die after a procedure at Waikato Hospital. Bob never got over her death.
Soulmates Bob and Carmen Walker on their wedding day. More than 50 years later Carmen would die after a procedure at Waikato Hospital. Bob never got over her death.
As the devastating news was being delivered the surgeon also exited the Harris Suite.
“He stood in the doorway and leant on the doorframe and basically didn’t say anything. And then they asked us if we’d like to go down to the Harris Suite,” Craig recalls.
“We went down and they just opened the door and they were basically still working on her and we just stood at the door.
“Then they took us into ICU and sat us down... and explained the situation was grave and ‘your mother’ is likely to pass on.”
There were various theories canvased during the inquest as to the cause of Walker’s estimated 2.5-litre blood loss - half her entire body’s blood.
These included leaking blood from the puncture wounds in the femoral artery, but pathologist Dr Ian Beer did not report obvious signs of bruising and swelling of the thigh or find any telltale blood.
The intensive care staff said Walker died of a massive gastrointestinal tract bleed, but Beer and expert forensic pathologist Dr Simon Stables said there was no sign of this at autopsy even though Beer went hunting for it based on the brief note he’d been given when he examined Walker’s body the next morning.
Greenbaum’s belief was that because of Walker’s calcified arteries and veins, the tourniquet was leaking, allowing blood from her body to slip into the leg unnoticed during the procedure and be drained along with the tainted blood and saline into the waste bucket during the exsanguination.
The problem with this was that Waikato Hospital did not have a measuring system in place and the fluid and other cytotoxic waste in the bucket was incinerated that night.
The nurse, who has name suppression, testified she queried whether to keep the waste but was told by a manager that because Walker didn’t die in theatre there was no need to. That policy still stands today, she said.
Meanwhile, notes that the surgeon made about the event were burned by him “about five years ago” in a bonfire.
By the time the Health and Disability Commissioner investigated, years had passed and everybody’s memories had begun to fade.
/cloudfront-ap-southeast-2.images.arcpublishing.com/nzme/6PMN22WW6NBUPEKBI5W2XD4LRY.JPG) Lance Walker promised his dying father Bob he'd get the truth of what happened to mum Carmen during the isolated limb infusion that went wrong at Waikato Hospital. Photo / Mike Scott
Lance Walker promised his dying father Bob he'd get the truth of what happened to mum Carmen during the isolated limb infusion that went wrong at Waikato Hospital. Photo / Mike Scott
The doctor who invented the ILI procedure and undertook 450 of them without any deaths, Professor John Thompson of Sydney, told the inquest the waste draining out of the venous line into the bucket should have been measured.
He believed Walker’s death was caused during the 14-minute wash-out, based on the haemoglobin of 28 and the empty heart.
Thompson added it was “most unusual” that the venous line was still heavily blood-stained after being washed with saline and following an unusually strong flow.
“The need for three attempts to clear the limb of residual blood using (the Rhys Davies exsanguinator) suggests continuing inflow of blood from the systemic circulation into the limb was occurring.”
When it was put to Thompson that each time the exsanguinator was pulled up the limb to the ankle it was drawing blood like a syringe from the rest of the body through a leaking tourniquet, before emptying the blood into the draining venous line, he said it was an “interesting concept”.
Justice for ‘Mum and Dad’
Walker was transferred to the ICU at 8pm. The anaesthetist commented it was unlikely she would survive the night.
Specialist anaesthetist Dr John Torrance, who was in charge of Walker’s intensive care told the inquest she would have required a number of treatments to survive such as dialysis and a colonoscopy.
He said because of the lengthy resuscitation it was likely she suffered severe brain damage and it would be “cruel” to save her only to live that way and succumb to cancer.
However, there was no chance to conduct a neurological assessment, to see if Walker had been trying to wake up.
The heparin had not been reversed meaning her blood could not clot.
Both anaesthetists said it was not appropriate to administer protamine in the ICU to clot her blood because this might have been the cause of the cardiac arrest.
“... in my view it would have been a reckless thing to have given protamine at that point,” the lead anaesthetist said.
She remained sedated and bled from the cannula sites and possibly her dying bowel as Torrance went home, leaving Walker’s care to a first-year registrar.
Fast-forward the clock 13 years.
With the inquest over, Craig, 69, and Lance, 63, are once more waiting, this time for the coroner to wade through thousands of pages of evidence, to make his findings and any recommendations. They are relieved Bob was no longer alive to witness the inquest.
“We’re going to have to let this process run its course and hope we get the truth basically,” Craig said.
“At the end of the day, to us, Mum bled out,” Lance said. “That’s what she died of. She had no blood left in her heart - where did it go?”
/cloudfront-ap-southeast-2.images.arcpublishing.com/nzme/GNAX2XREPZBGLAN6TXU4SXYJ4M.jpg) Carmen Walker with sons Craig (left) and Lance Walker long before Carmen's tragic death.
Carmen Walker with sons Craig (left) and Lance Walker long before Carmen's tragic death.
The inquest process had been gruelling, dredging up the grief and anger they’d dealt with previously but they attended every day because it was about “getting justice” for their parents.
Of the witnesses, they felt some were invested in protecting their reputations and gave “well-scripted” testimony, leaving a question mark in their minds over how genuine their evidence was.
The brothers wanted name suppressions lifted.
“I think they carry on like they’re beyond reproach,” Craig said.
“I get the impression they think they’re untouchable,” Lance said. “These guys are professionals. The general public puts their life in their hands and they expect to get the best.”
Natalie Akoorie is the Open Justice deputy editor, based in Waikato and covering crime and justice nationally. Natalie first joined the Herald in 2011 and has been a journalist in New Zealand and overseas for 27 years, recently covering health, social issues, local government, and the regions.

Take your Radio, Podcasts and Music with you









